
Towards a potential role of beta-blockers in future cancer treatment - filling the gaps
We hypothesize that beta-blockers, which perturb the β-adrenergic axis, can boost the standard of treatment; thereby turning prostate cancer into a chronic disease at a reasonable cost, both for the patient and the health care providers.
We were the first to show that use of beta-blockers is associated with reduced prostate cancer specific mortality using data from the Cancer Registry of Norway, The Cause of Death Registry and the Norwegian Prescription Database. Our focus is now to determine the potential of beta-blockers to improve therapy response using epidemiological data and various pre-clinical models. The effects of adrenergic signalling on cancer cells and the tumour microenvironmen will be unravelled. This will give us knowledge about whether, when and why beta-blockers have a positive effect on therapy response.
- Determine whether beta-blockers use is associated with progression during therapy using national registries (Shivanthe Sivanesan and Helene Hartvedt Grytli)
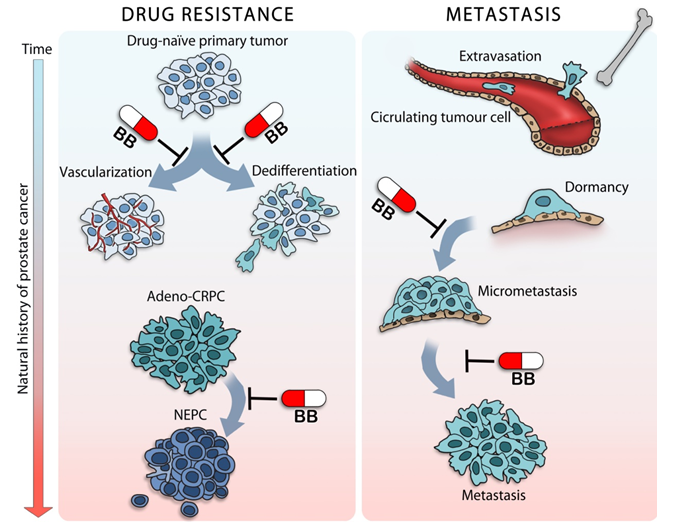
- Determine whether beta-blockers improve the effect of drugs targeting the androgen axis using model systems developing CRPC (Heidi Kristin Nielsen and Helene Hartvedt Grytli)
- Determine whether and how beta-blockers inhibit development of neuroendocrine prostate cancer using preclinical model systems (Peder Rustøen Braadland)
Based on analysis of patient data and preclinical mechanism studies described in this project, we will with high probability be able to predict which patient group will be most likely to benefit from beta-blockers and which treatment regimen that should be initially tested. This will lay the foundation for a clinical trial.
We suggest that by complementing the toolbox with beta-blockers s, we will be able to prolong therapy responses and thereby transform lethal prostate cancer into a chronic disease in a subgroup of patients.
The concept of repurposing out-of-patent drugs for treatment of cancer is a desirable approach. By this approach, time and money are saved during development, the cost of use is low, and there is a pile of safety data that have been collected over many years.
Can beta-blocker treatment reduce cancer recurrence after radical prostatectomy?
Aim:
Investigate if there is epidemiological evidence supporting neo-adjuvant beta-blocker use prior to radical prostatectomy
Why:
- More than 1000 men undergo radical prostatectomy for prostate cancer in Norway, making surgery the most common treatment option for prostate cancer.
- About one-third experience cancer recurrence after radical treatment.
- There is an increasing amount of epidemiological evidence supporting the association between beta-blocker use and prostate cancer specific survival (link til intern side).
- There are ongoing clinical studies evaluating perioperative beta-blocker use in other cancer types.
How:
- More than 11000 men radically operated for prostate cancer were identified in the database atthe Cancer Registry of Norway.
- Data from the Cancer Registry of Norway were coupled to information from the Norwegian Prescription Database, Norwegian Patient Registry and Norwegian Cause of Death Registry.
- The associations between beta-blocker use and cancer recurrence are studied using multi-variate analyses.
- Sub-analyses addressing the effect of various types of beta-blockers, timing and interference of other medications are on-going.
Future plans:
Validate the results using data from the Radical Prostatectomy Registry at Oslo University Hospital.
Evaluate the possibility for a pilot RCT.
Project members: Shivanthe Sivanesan, Helene Hartvedt Grytli