
Selected projects
Lower than expected burden of premature ventricular contractions impairs myocardial function
Lie OH, Saberniak J, Dejgaard LA, Stokke MK, Hegbom F, Anfinsen O-G, Edvardsen T, Haugaa KH
Frequent premature ventricular contractions (PVCs) can induce myocardial dysfunction. Patients with outflow tract arrhythmia (OTA) commonly have frequent PVCs without structural heart disease. In this study we aimed to explore the burden of PVCs associated with myocardial dysfunction in patients with OTA. We hypothesized that this threshold is lower than the previously suggested threshold of 24 000 PVCs/24 h (24%PVC) when systolic function is assessed by strain echocardiography. Furthermore, we aimed to characterize OTA patients with malignant arrhythmic events. We included 52 patients referred for OTA ablation. Left ventricular global longitudinal strain (GLS) and mechanical dispersion were assessed by speckle tracking echocardiography. A subset underwent cardiac magnetic resonance imaging. PVC burden (%PVC) was assessed by Holter recordings and reported as the percentage of total heart beats. Sinus rhythm QRS durations and PVC QRS durations were recorded from 12-lead electrocardiogram, and the QRS ratio was calculated (PVC QRS duration / sinus rhythm QRS duration). %PVC correlated with GLS with mechanical dispersion, but not with ejection fraction. %PVC was higher in patients with impaired systolic function by GLS (worse than -18%) compared with patients with normal function. Greater than 8%PVC optimally identified patients with abnormal GLS. Serious arrhythmic events occurred in 11 (21%) patients. These were characterized by high QRS.
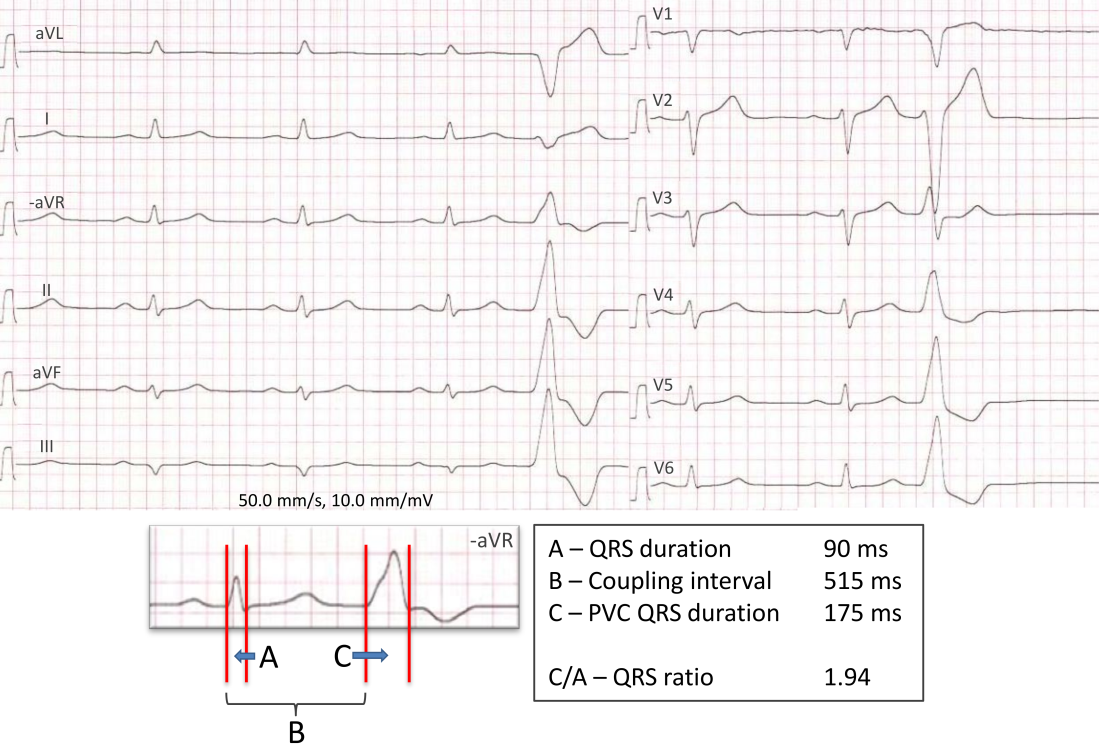
Figure: Outflow tract arrhythmia on the electrocardiogram. Twelve-lead electrocardiogram of patient X with outflow tract arrhythmia and history of sustained ventricular tachycardia and syncope. There is dominating left bundle branch block morphology and inferior electrical axis of the premature ventricular contraction (PVC), and the QRS ratio, calculated by dividing the PVC QRS duration (C) by the sinus rhythm QRS duration (A), is > 1.9. This is suggestive of a right ventricular outflow tract-free wall PVC origin. By Holter recording, this patient had 33% PVCs. From Lie OH, Saberniak J, Dejgaard LA, et al. Lower than expected burden of premature ventricular contractions impairs myocardial function. ESC Heart Fail 2017;4(4):585-94
Prognostic Value of Left Ventricular Deformation Parameters in Patients with Severe Aortic Stenosis: A Pilot Study of the Usefulness of Strain Echocardiography
Klaeboe LG, Håland TF, Leren IS, Bekke R, Brekke PH, Røsjø H, Omland T, Gullestad L, Aakhus S, Haugaa KH, Edvardsen T
In aortic stenosis, subtle alterations in myocardial mechanics can be detected by speckle-tracking echocardiography prior to reduction of left ventricular ejection fraction (LVEF). In this prospective study, 162 patients with severe aortic stenosis and preserved LVEF (60 ± 11%) were included. Surgical aortic valve replacement was performed in 120 patients, whereas 42 were deemed ineligible for surgery. Mechanical dispersion was pronounced (64 ± 20 msec) in the total patient population.
Pronounced mechanical dispersion at baseline was a predictor of mortality in patients with severe aortic stenosis independently of LVEF, flow status, or treatment (AVR vs medical treatment), providing incremental prognostic information in addition to LVEF, GLS, and correlates of flow and gradient.
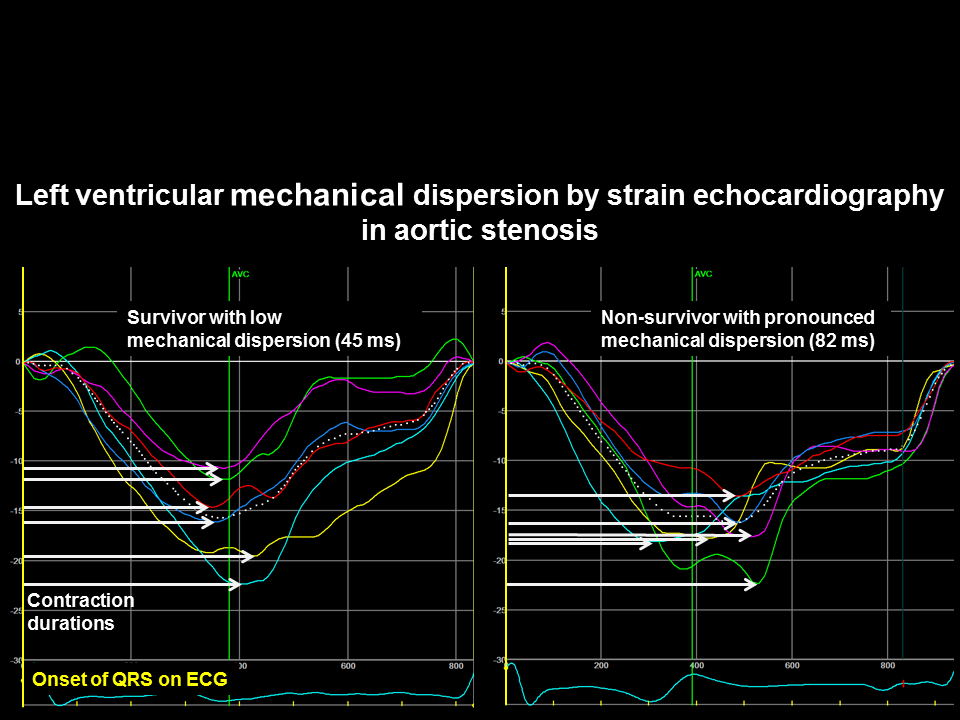
Figure: Speckle-tracking echocardiography showing longitudinal strain curves in the four-chamber view from patients with aortic stenosis demonstrating a more homogenous contraction pattern (lower mechanical dispersion) in a survivor than in a nonsurvivor (pronounced mechanical dispersion). From Klaeboe et al. J Am Soc Echocardiogr 2017;30:727-735.e1