Sarcomas of the uterus
So far there are 500 patients included in this study. Again we will test DNA-ploidy and nucleotyping as diagnostic/predictive value. In addition we will make a TMA using all of the samples in the study.
Read about the background for our projects:
Large scale genomic instability
We have several projects going on the following material:
| FCM \ ICM | Diploid | Tetraploid | Polyploid | Aneuploid | Sum |
| Diploid | 85 | 29 | 4 | 12 | 130 |
| Tetraploid | 12 | 4 | 15 | 31 | |
| Polyploid | 1 | 1 | |||
| Aneuploid | 9 | 4 | 1 | 54 | 68 |
| Sum | 94 | 45 | 10 | 81 | 230 |
")
These projects are more or less finished:
Projects we work with at present:


| Flow cytometry | Image cytometry |
| Sectioning (100mm) | Sectioning (50mm) |
| Deparaffination | Deparaffination |
| Enzyme treatment (pepsine, RNase) | Enzyme treatment (protease) |
| Cytospin centrifugation (monolayer) | |
| Staining with ethidium bromide | Staining with feulgen-schiff |
| Measurements | Measurements |
| Flow cytometry | Image cytometry | |
| Advantages | Fast | Morphological control |
| Disadvantages | No morphological control | Time-consuming |
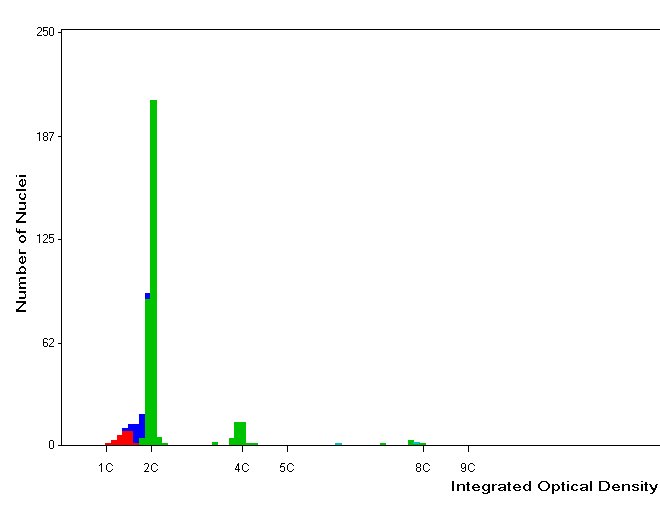
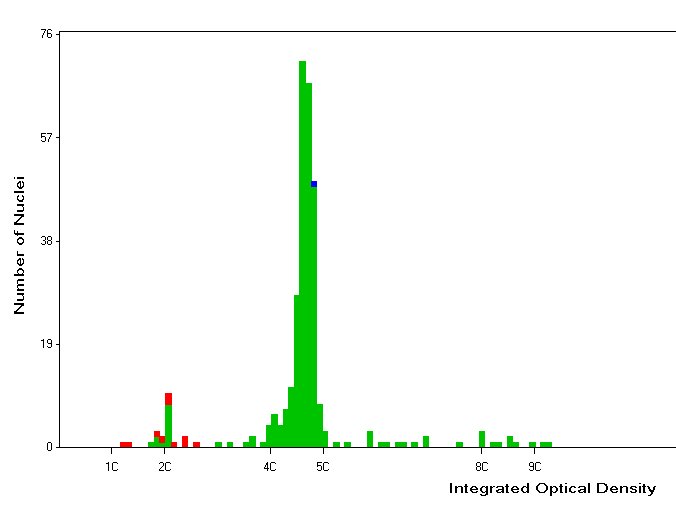
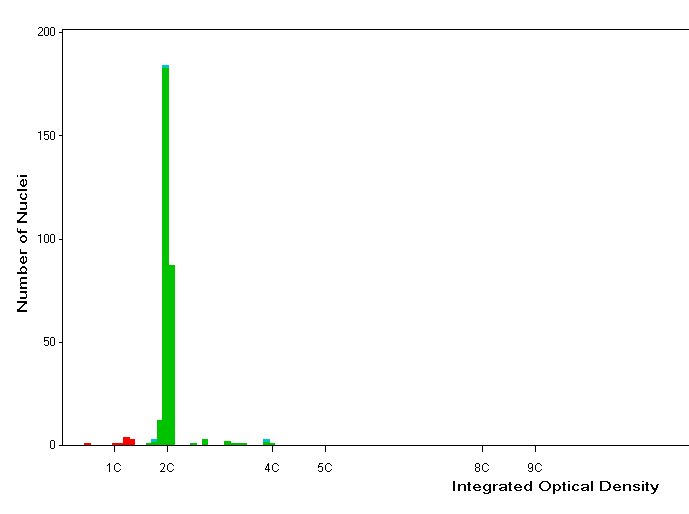
| Diploid | Tetraploid | Aneuploid |


We have two main projects on cancer mammae:
CCIS Study
Ductal Carcinoma in situ represents certain challenges in diagnostics, because around 20 % develop into invasive cancer and there are no certain markers to identify these. We have analysed a number of samples using both DNA ploidy and nucleotyping.
Mammae cancer, stadium I
In this case we have a total of 480 patients with a defined prognosis (good prognosis: no relapse > 7 years after treatment. Bad prognosis: relapse or death of cancer within 4 years). The study is a pilot for DNA ploidy and nucleotyping as a prognostic marker in breast cancer. There are also planned to do a comparison of alternative methods for DNA ploidy measurements (FCM, manual ICM, automated ICM) and S-phase calculations.